Modern operating rooms are faster, busier and more technologically advanced than ever before.
But as surgical throughput increases and experienced perioperative clinicians leave the workforce, many healthcare professionals are asking an important question:
Are the fundamentals of aseptic technique and sterile workflow being unintentionally diluted?

Operating rooms today are under immense pressure:
- increasing surgical demand
- workforce shortages
- rapid turnover expectations
- rising procedural complexity
- growing technology integration
Yet despite these pressures, one principle remains unchanged:
Every movement in the operating room matters.
The Operating Room Is a Workflow Environment
Aseptic technique is not simply about sterile gloves and gowns.
It is a coordinated clinical workflow built around:
- movement discipline
- contamination prevention
- environmental awareness
- communication
- surgical conscience
- team coordination
The way perioperative staff:
- open sterile supplies
- move around sterile fields
- don masks and PPE
- position equipment
- manage cables and robotics
- control theatre traffic
- protect sterile setups
all contribute directly to infection prevention and patient safety.
These behaviours are often learned not from policy alone, but through:
- mentorship
- observation
- repetition
- correction
- supported perioperative education
“Aseptic technique is not just taught. It is passed on.”
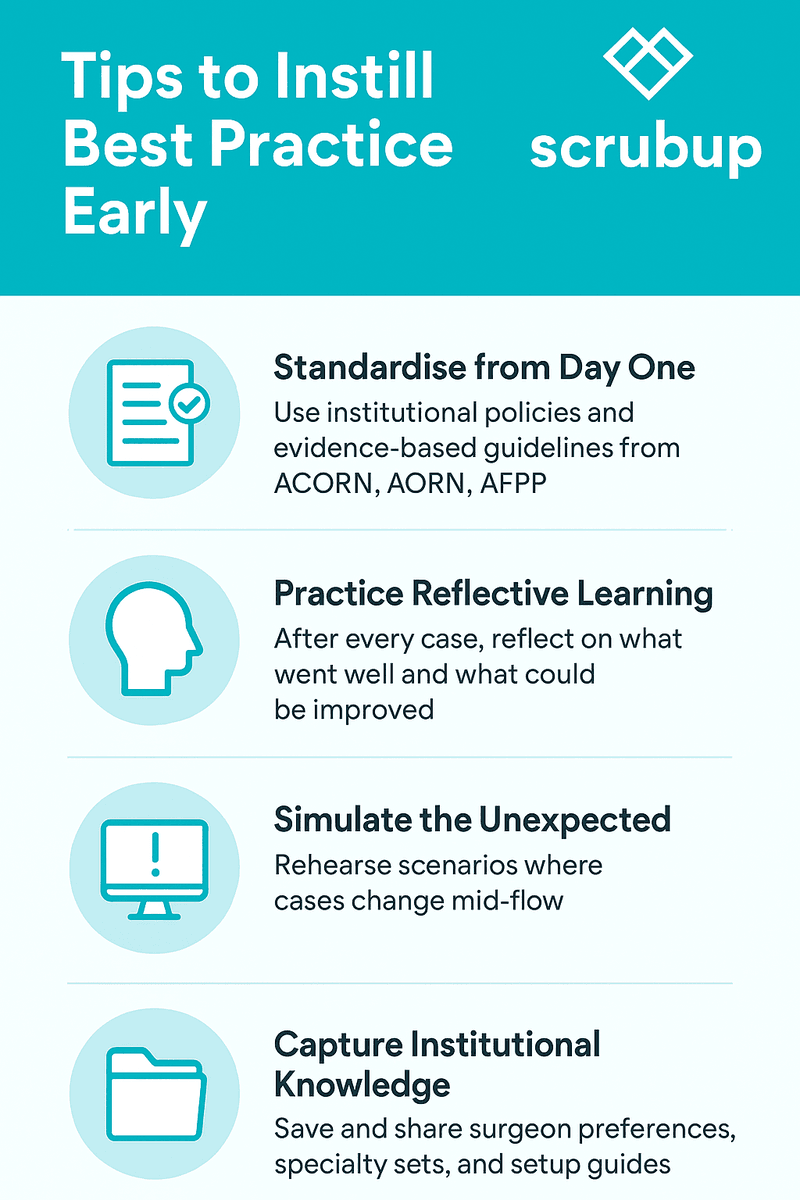
International Perioperative Standards Exist for a Reason
Globally recognised perioperative organisations including:
- Association of periOperative Registered Nurses (AORN)
- Australian College of Perioperative Nurses (ACORN)
- Operating Room Nurses Association of Canada (ORNAC)
- European Operating Room Nurses Association (EORNA)
have developed standards and guidelines to support:
- aseptic technique
- sterile field management
- operating room traffic control
- surgical attire and masking
- environmental cleaning
- patient preparation
- surgical hand antisepsis
- sterile supply handling
- infection prevention and control
These standards exist because variability in sterile practice increases risk.
They reinforce principles such as:
- never walking between two sterile fields
- maintaining sterile boundaries
- reducing unnecessary door openings
- minimising operating room traffic
- correct sterile opening technique
- maintaining visual awareness of sterile items
- appropriate mask use in restricted areas
- protecting airflow integrity
Yet maintaining these standards consistently requires:
- education
- reinforcement
- supervision
- competency development
- perioperative culture

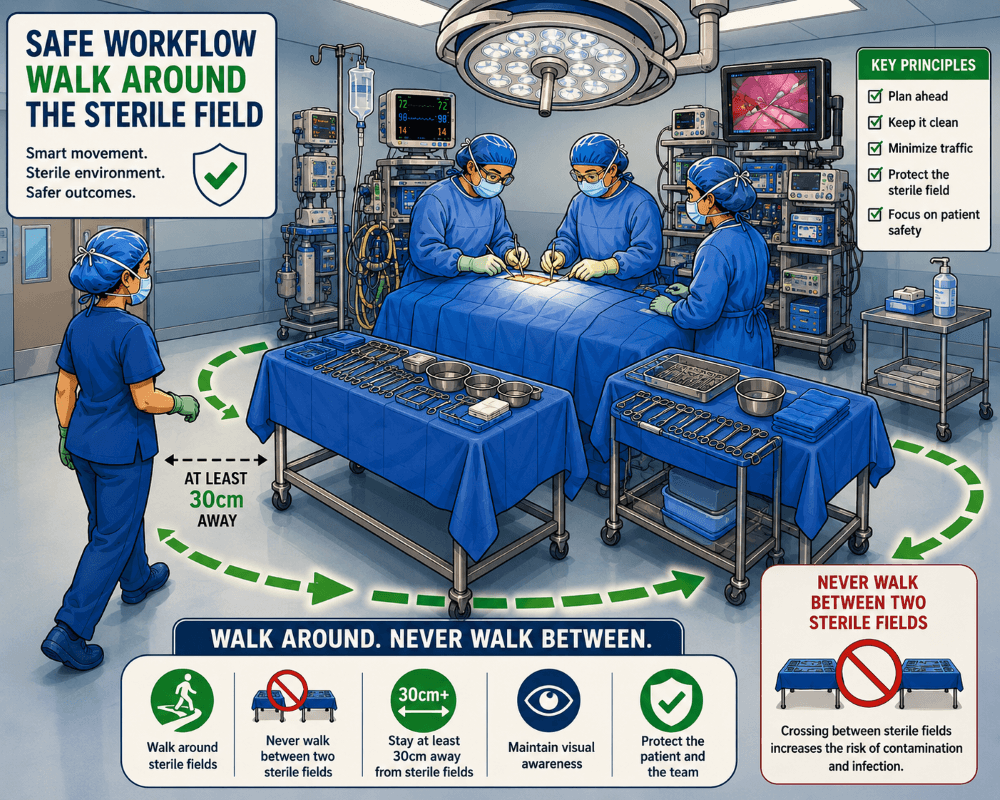
Every Movement Around a Sterile Field Matters
Many perioperative clinicians remember being taught:
- to walk around sterile fields
- not between two sterile setups
- never turn your back on an open sterile trolley
- avoid reaching over sterile equipment
- maintain clean-to-dirty workflow
- protect sterile boundaries at all times
These principles may appear simple.
But they are critical infection prevention behaviours developed over decades of perioperative practice.
Clinical workflow examples include:
- circulator nurses walking around sterile fields to adjust room equipment
- correct opening of sterile supplies without contaminating contents
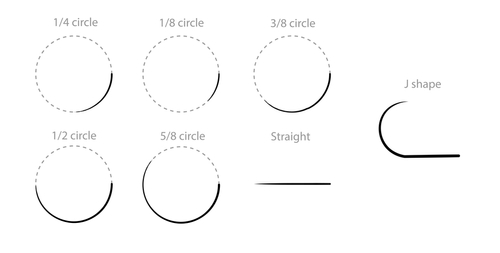
- safe handling of sterile instruments
- controlled patient skin preparation techniques
- minimising airflow disruption
- maintaining sterile awareness during robotic surgery setup
- safe positioning of equipment and cables around the sterile field
“The basics are not basic. They are the invisible safety systems that protect patients every day.”
Throughput Pressure May Be Reducing Teaching Opportunities
Modern operating rooms are balancing:
- efficiency targets
- staffing shortages
- increased case complexity
- onboarding of novice staff
- rapid orientation requirements
- increasing reliance on temporary workforce models
Under these conditions, perioperative education can unintentionally become compressed.
Yet many of the most important sterile workflow skills are experiential.
Learning:
- how to safely circulate around a sterile field
- how to recognise subtle contamination risks
- how to safely open sterile consumables
- how to protect a sterile setup during room movement
- how to anticipate contamination before it occurs takes time, mentorship and repetition.
Research examining missed nursing care in Australia in perioperative settings identified workload, organisational and communication pressures contributing to omitted or delayed care activities. These pressures may indirectly affect sterile workflow vigilance and education opportunities.
Infection Prevention Starts Before the Incision
Infection prevention begins long before surgery starts.
It begins with:
- correct patient preparation
- appropriate PPE use
- sterile equipment setup
- environmental control
- disciplined operating room workflow
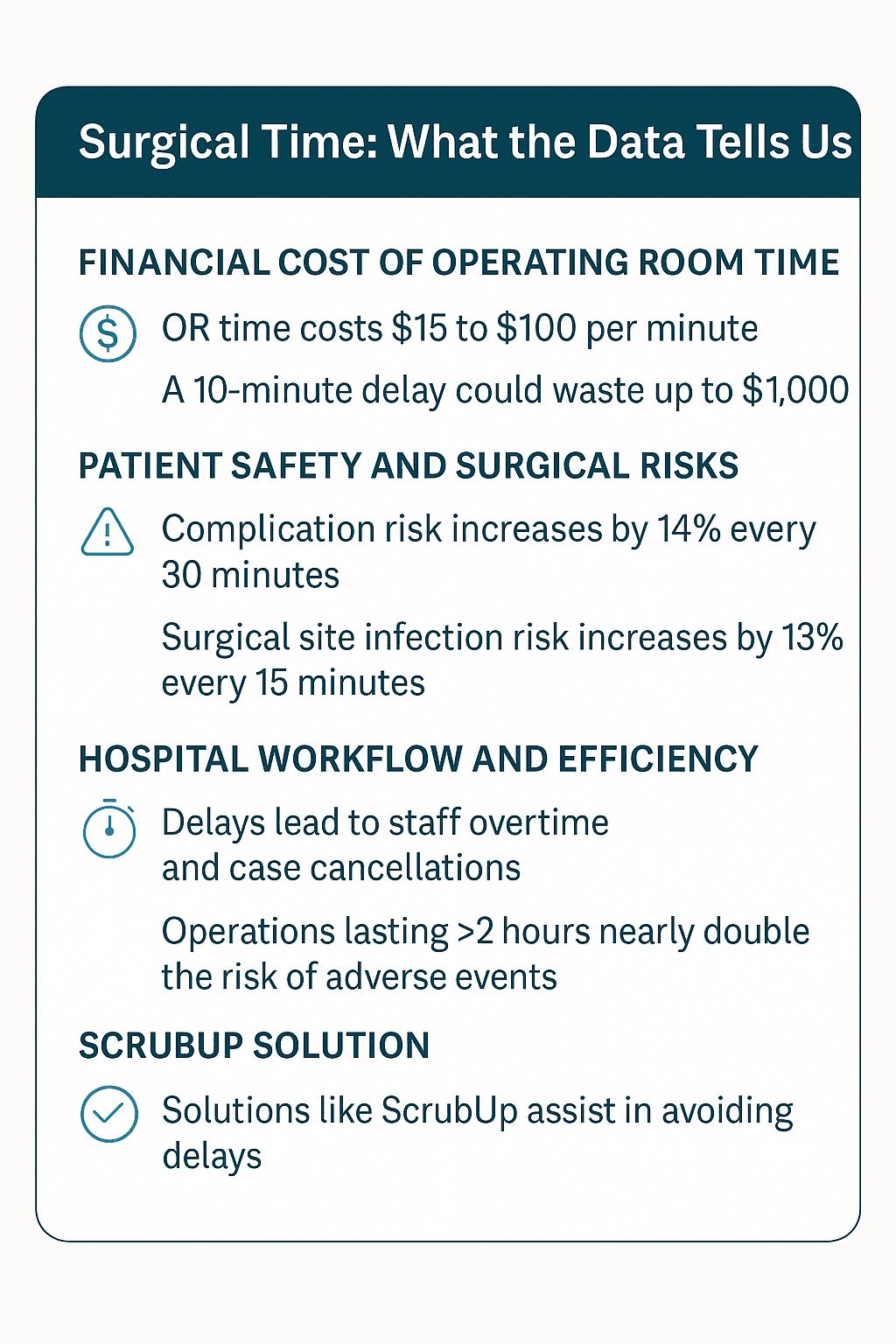
Research has demonstrated associations between:
- operating room traffic
- door openings
- airflow disruption
- microbial contamination risk
- surgical site infection risk
A 2025 systematic review identified evidence suggesting increased operating room door openings may contribute to increased surgical site infection risk.
Another study found that increased theatre traffic and longer surgical duration were associated with increased airborne microbial contamination within operating rooms.
These findings reinforce an important principle:
Human behaviour within the operating room environment matters.
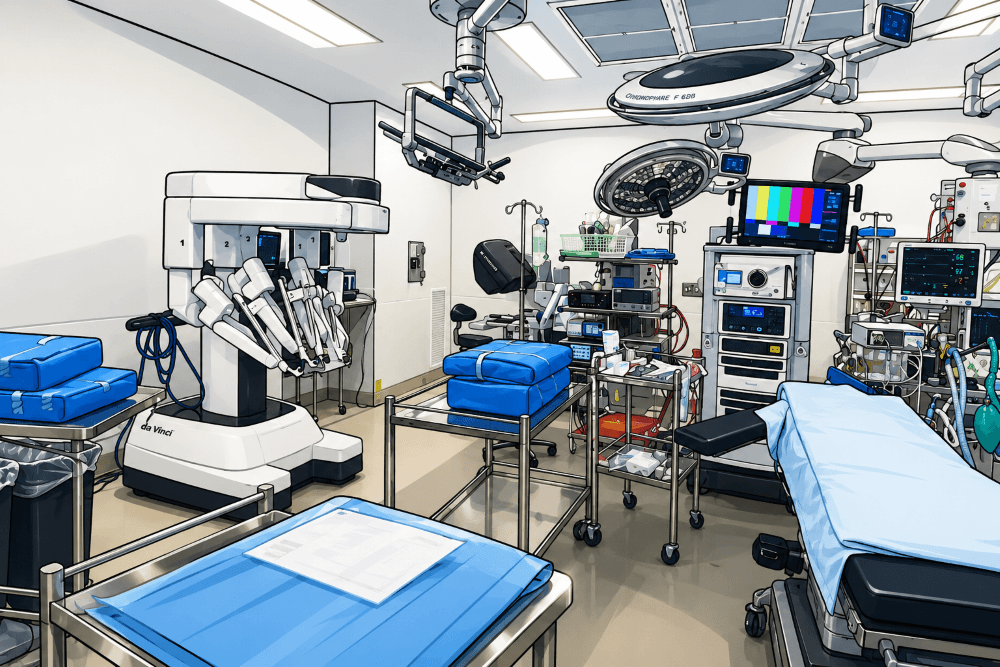
Modern Operating Rooms Are Becoming More Complex
Today’s perioperative environments include:
- robotic surgery systems
- advanced imaging integration
- multiple digital platforms
- increased equipment density
- complex cable management
- multidisciplinary workflow coordination
While technology supports surgical advancement, it also increases cognitive and workflow complexity.
This makes strong perioperative education more important than ever.
Because technology alone cannot replace:
- sterile awareness
- workflow discipline
- situational awareness
- contamination anticipation
- perioperative teamwork
Surgical Conscience Must Be Protected
Historically, perioperative culture has relied heavily on experienced clinicians passing on sterile discipline to the next generation.
This includes:
- correcting unsafe movement
- reinforcing sterile awareness
- teaching contamination prevention
- supporting psychological safety
- encouraging staff to speak up
When experienced perioperative clinicians leave without structured succession and mentorship, organisations risk losing:
- institutional knowledge
- workflow discipline
- contamination prevention behaviours
- confidence within teams
- perioperative culture itself
Key Concerns Facing Modern Operating Rooms
- Reduced perioperative orientation time
- Increased surgical throughput pressure
- Loss of experienced perioperative clinicians
- Reduced mentorship opportunities
- Workflow interruptions
- Increased operating room traffic
- Cognitive overload
- Inconsistent aseptic technique reinforcement
- Increased technology complexity
- Pressure to prioritise efficiency over education
Why This Matters
- Surgical site infections remain a significant global patient safety concern.
- Operating room traffic and door openings have been associated with increased contamination risk.
- Missed perioperative nursing care has been linked with workload and communication pressures.
- Perioperative workflow directly influences sterile field protection.
- Replacing experienced perioperative clinicians is costly and time intensive.
- International perioperative standards exist to reduce preventable harm and support safe surgical practice.
The Future of Safe Surgery Depends on the Basics
Modern surgery will continue to evolve through:
- robotics
- digital integration
- advanced technology
- artificial intelligence
- complex procedural innovation
But no technology can replace:
- surgical conscience
- sterile awareness
- disciplined workflow
- perioperative mentorship
- human vigilance
The future of safe surgery will not depend solely on innovation.
It will depend on whether we continue to protect and teach the fundamentals that keep patients safe every single day.
Because the basics are not “basic.” They are the foundation of safe perioperative care.
References
- Gillespie BM, Harbeck E, Kang E, et al. Missed nursing care in Australian perioperative settings: A cross-sectional study. Journal of Advanced Nursing. 2024. Available at: https://pubmed.ncbi.nlm.nih.gov/38380764/
- Blomberg AC, Lindwall L, Bisholt B. Operating room nurses’ experiences of maintaining aseptic technique and safe practice in the surgical environment. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC12465459/
- Dancer SJ, et al. Operating room door openings, microbial contamination and surgical site infection risk: systematic review. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC12159596/
- Andersson AE, Bergh I, Karlsson J, Nilsson K. Traffic flow in the operating room: an explorative and descriptive study on air quality during orthopedic trauma implant surgery. American Journal of Infection Control. 2018. Available at: https://www.ajicjournal.org/article/S0196-6553(18)30156-1/pdf
- Gillespie BM, et al. Simulation-based patient safety education for perioperative clinicians: improving safety competencies and teamwork. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC10649324/
- Scoping Review of Aseptic Technique Definitions and Practices in Healthcare Settings. International Journal of Nursing Practice. 2025. Available at: https://www.sciencedirect.com/science/article/pii/S019567012500266X
- Joint Commission International. Surgical Site Infection Prevention Toolkit. Available at: https://digitalassets.jointcommission.org/api/public/content/assets/3/7/jci_ssi_toolkit.pdf
- AORN Guidelines for Perioperative Practice — Association of periOperative Registered Nurses
- ACORN Standards for Perioperative Nursing in Australia — Australian College of Perioperative Nurses
- ORNAC Standards and Recommended Practices — Operating Room Nurses Association of Canada
- EORNA European Perioperative Guidelines and Resources — European Operating Room Nurses Association